In vitro fertilization (IVF) involves fertilization outside the body in an artificial environment. IVF was first successfully used for human infertility in 1977 at Bourne Hall in Cambridge, England. To date, tens of thousands of babies have been delivered worldwide as a result of IVF treatment. Over the years, the procedures to achieve IVF pregnancy have become increasingly simpler, safer and more successful.

In Vitro Fertilization (IVF)
The IVF process has several steps:
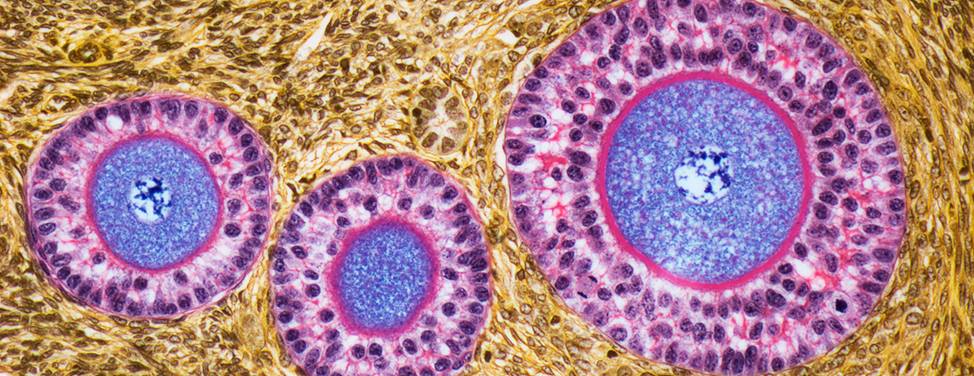
- Stimulation of the ovary to produce several fertilizable oocytes (eggs)
- Retrieval of the oocytes from the ovary
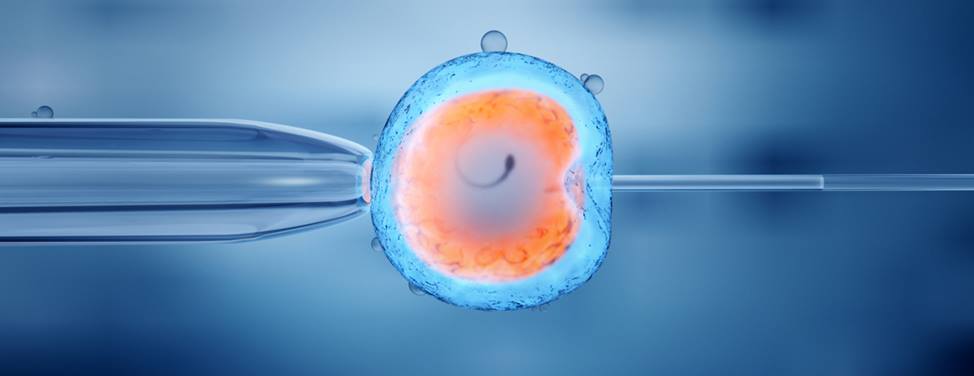
- Fertilization of the oocytes and culture of the embryos in the IVF laboratory
- Placement of the embryos into the uterus for implantation (embryo transfer or ET)
IVF may be useful for the following types of problems:
- Absent fallopian tubes or tubal disease that cannot be treated successfully with surgery
- Endometriosis that has not responded to surgical or medical treatment
- Male infertility with low sperm counts or motility, but with enough active sperm to allow fertilization in the laboratory
- Severe male factor infertility in which sperm must be obtained surgically
- Unexplained infertility that has not responded to other treatments
- Genetic diseases that result in miscarriage or abnormal births
In addition to standard IVF procedures – including intracytoplastmic sperm injection, assisted hatching, and blastocyst culturing – we offer a more unique technique, called embryo co-culture. In embryo co-culture, embryos are grown in "feeder layers" of cells from the patient that enhance development. This technique appears to improve embryo growth for patients who have had poor embryo development and unsuccessful IVF cycles.
Continue reading
Assisted Hatching
In assisted hatching, a laser is used to thin the zone pellucida (outer shell) of the fertilized egg before it is transferred into the uterus. This outer shell is believed to become thicker and hardened with aging of the oocyte (egg).
Women of advanced age, or with an elevated follicle stimulating hormone (FSH) level on day three, may have decreased chance for embryo implantation. The embryos of women with endometriosis and poor quality embryos may also have this problem. The assisted hatching technique was introduced to enhance the embryos' ability to hatch, and thus implant, after transfer.
You may be a candidate for assisted hatching if you are 38 years of age or older, have an elevated basal FSH level, or if you have previously had one or more IVF cycles in which your embryos failed to implant, despite otherwise good results.
Blastocyst Culturing
Blastocyst culturing is a technique to grow embryos beyond the third day of culture. Typically with IVF, embryos are transferred into the uterus about three days after the egg retrieval. On the third day, embryos generally are between six to eight cells. Over the years, improved culture environments have allowed us to culture the embryos two additional days. During this additional culture period, the embryos continue to grow to become "blastocysts."
The natural process of embryo development begins with the fertilization of the egg in the outer aspect of the fallopian tube. As the newly formed embryo develops, it moves slowly toward the uterine cavity where it will ultimately implant. This process takes approximately six to seven days. When the embryo reaches the "blastocyst" stage, it is ready to implant.
In certain patients, blastocyst culturing allows optimal selection of embryos for transfer, resulting in an increased implantation rate per embryo transferred. However, it is important to understand that this technology may not necessarily increase your chance for pregnancy. The main advantage is that fewer embryos may be transferred to eliminate the possibility of multiple pregnancies, while maintaining a high pregnancy rate.
Generally speaking, this procedure should be limited to patients with excessive numbers of embryos – more than five – in which case further selection of embryos beyond the day three stage would be advantageous. As a general rule, patients under age 37 are candidates for this culturing technique.
For younger patients, up to 50 percent of all embryos will continue to grow to the blastocyst stage. However, 10 percent of patients won't have an opportunity for embryo transfer due to the absence of blastocyst development. As patients get older, fewer and fewer numbers of embryos are capable of developing in culture to the blastocyst stage.
Embryo Co-Culturing with Endometrial or Granulose Cells
Embryo co-culturing is a technique used to improve the overall quality of embryos before transferring them into the mother's uterus. It was initiated in the UCSF IVF Laboratory, but several other IVF programs in the world have used this technique since 1996. Co-culturing uses human granulosa or endometrial cells that may secrete nutritional products that help growing embryos improve their chances for survival.
Using co-culturing, we have seen an improvement in embryo quality and relative growth 72 hours after egg retrieval. Eggs fertilize within 18 to 24 hours after egg retrieval.
We only recommend this technique to patients who have had previous unsuccessful IVF cycles with poor embryo quality, either here at UCSF or with another program. We do not recommend it to patients who have never been through IVF before, or who have had treatment cycles with excellent embryo quality in the past.
An important concept to understand is that your likelihood of achieving pregnancy, regardless of your age, depends on the overall quality of your embryos. If you have generally good embryo quality, then you have a higher chance of conceiving from your IVF treatment cycle. Conversely, if you have generally poor embryo quality, then your chance for success diminishes.
The risks associated with co-culture are unknown at this time. Because it has never been tested extensively, there is no information regarding children born of co-culture using these specific cells. Because of this fact, we remain cautious about using this technique on patients who clearly may not benefit from it. It is important to understand that some patients may not have improved embryo quality, despite the use of co-culturing.
If you and your doctor agree to use co-culture for your IVF treatment cycle, then we will incubate all your embryos in the co-culture environment as soon as our embryologists confirm fertilization. We will continue co-culture until the day of your embryo transfer.
It is possible to freeze co-culture embryos. Co-culture will not affect the ability of your embryos to freeze well. We use the same standards for freezing co-cultured embryos as we do for standard cultured embryos. If your embryo quality is improved with co-culture, there is a greater likelihood that we will be able to freeze more embryos for you.
UCSF Health medical specialists have reviewed this information. It is for educational purposes only and is not intended to replace the advice of your doctor or other health care provider. We encourage you to discuss any questions or concerns you may have with your provider.