FAQ: Intracytoplasmic Sperm Injection
- What is ICSI?
- Who should consider ICSI?
- Who should consider split ICSI?
- How successful is ICSI?
- What are the risks associated with ICSI?
- Will all of our eggs be injected?
- Are there differences in embryo quality or pregnancy rates between ICSI and non-ICSI embryos?
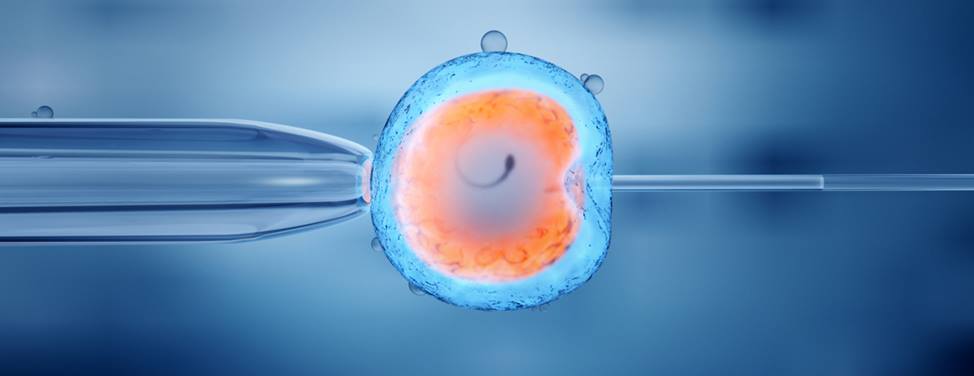
What is ICSI?
Intracytoplasmic sperm injection, or ICSI, involves injecting a single live sperm directly into the center of a human egg. The technique was developed to help achieve fertilization for couples with severe male factor infertility or couples who have had failure to fertilize in a previous in vitro fertilization (IVF) attempt. The procedure overcomes many of the barriers to fertilization and allows couples with little hope of achieving successful pregnancy to obtain fertilized embryos.
The procedure requires that the female partner undergo ovarian stimulation with fertility medications so that several mature eggs develop. These eggs are then aspirated through the vagina using vaginal ultrasound, and incubated under precise conditions in the embryology laboratory. The semen sample is prepared by centrifuging, or spinning the sperm cells through a special medium. This separates live sperm from debris and most of the dead sperm. The embryologist then picks up the single live sperm in a glass needle and injects it directly into the egg.
ICSI was first used at UCSF in 1994, and our first successful birth achieved with ICSI assistance was in February of 1995. UCSF was the first San Francisco Bay Area program to achieve a pregnancy and birth with this procedure.
Who should consider ICSI?
ICSI is considered absolutely necessary is in the case of male factor infertility with an abnormal semen analysis. In the Bay Area, however, about 75 percent of all IVF cases are now ICSI. Patients are electing to undergo ICSI for reasons other than male factor infertility, including:
- Previous poor fertilization with IVF
- Variable sperm counts
- Unexplained infertility
Many patients choose to undergo the ICSI procedure in order to maximize their success even when the procedure is not clearly indicated.
If you have been told that there are abnormalities with any sperm test results, you should give serious consideration to ICSI. If the male partner has had a vasectomy reversal, we also recommend ICSI regardless of the sperm quality because of the presence of sperm antibodies that may affect fertilization.
The decision to proceed with ICSI is particularly difficult if there is no prior evidence of male factor infertility. Some couples choose ICSI because they want to do everything possible to maximize fertilization. However, it is important to understand that for many couples with normal sperm parameters, maximal fertilization can be achieved with standard insemination during IVF without the use of ICSI.
Who should consider split ICSI?
For couples interested in knowing about their own fertilization capability, we offer split ICSI. This option involves performing ICSI on a majority of all mature eggs and incubating the remainder with sperm. In effect, split ICSI can provide a safety net against failed fertilization with standard insemination.
The fee charged for split ICSI is the same as ICSI. One requirement for split ICSI is a minimum number of mature eggs. We must be able to identify at least eight mature eggs on the day of your egg retrieval in order to proceed with split ICSI. If this requirement is not met, we will inject all of your mature eggs.
How successful is ICSI?
Through the ICSI procedure, many couples with difficult male factor infertility problems have achieved pregnancy at UCSF. Fertilization rates of 70 to 80 percent of all eggs injected – equivalent to fertilization with normal sperm – are currently being achieved, and pregnancy rates are comparable to those seen with IVF in couples with no male factor infertility.
The most important indicator of ICSI success appears to be the fertilization rate achieved with the ICSI procedure. The fertilization rate in the UCSF IVF laboratory is exceptional – currently 80 to 85 percent. That is to say, on average, eight out of every 10 eggs will fertilize normally.
What are the risks associated with ICSI?
There are several risks. First, during the ICSI procedure, a small number of eggs – usually less than 5 percent – can be damaged as a result of the needle insertion. Second, the overall risk of having a baby with a chromosomal abnormality in the X or Y chromosomes is 0.8 percent, or eight per 1000, which is four times the average seen with spontaneous conception. At present, we do not know the reason for this increased risk.
It is important to understand that the following problems can be associated with sex chromosome abnormalities:
- Increased risk of miscarriage
- Heart problems for affected infants that may require surgery
- Increased risk of behavior or learning disabilities
- Increased risk of infertility in your children during their adulthood
The risk of having a chromosomal abnormality like Down's syndrome is not increased with ICSI but increases with maternal age.
Several studies have addressed the issue of developmental delays in children born of ICSI. However, there is no conclusive evidence that this is the case.
Will all of our eggs be injected?
If you decide to proceed with ICSI, we will make every effort to inject as many eggs as possible. It is important for you to understand that only eggs that are mature can be injected with sperm. Our IVF laboratory can easily tell if an egg is mature or immature. Although the immature eggs are incubated with sperm, the likelihood of fertilization is very low. On average, we are able to inject 75 percent to 80 percent of the eggs that are recovered.
Are there differences in embryo quality or pregnancy rates between ICSI and non-ICSI embryos?
There appears to be no difference in the overall embryo quality achieved with ICSI embryos when compared to non-ICSI embryos. Similarly, no difference in pregnancy rates has been shown between ICSI embryos and non-ICSI embryos. Although unproven, there is a belief among many infertility specialists that ICSI may increase embryo yield from a given number of eggs recovered, which has contributed to the increase in ICSI procedures.
UCSF Health medical specialists have reviewed this information. It is for educational purposes only and is not intended to replace the advice of your doctor or other health care provider. We encourage you to discuss any questions or concerns you may have with your provider.